Ashley
ashy_toasty
about
Ashley, Ash, Ashy
she/her
28 y.o.
bisexual, married💍
Dallas, TX, U.S.A.
Certified Pharmacy Technician (CPhT) --- aka badaṣṣ; since 2014
B.A. in Psychology ('18) --- Summa Cum Laude, with honors
M.S. in Clinical Psychology with a specialization in Neuropsychology ('21)
bisexual advocate
mental health advocate
Hodgkin's lymphoma survivor (cancer)
ADHD, BPD (rule out), suspecting autism
cat mom
interests
psychology
mental health
true crime
health science
pharmacology
Bazzi
blackbear
Halsey
Krewella
ReadyToGlare
Stephanie Harlowe
Brooke Makenna
Bailey Sarian
Kendall Rae
Sam Collins
Danelle Hallan
Molly Burke
Mama Doctor Jones
Glam & Gore
Doctor Mike
AnthonyPadilla
Good Mythical Morning
Twin Paranormal
Smosh

Animal Crossing: New Horizons
Forza Horizon 3 & 4
Mario Kart
Sims 4
Toontown Rewritten

personality
mom friend
INTJ
fluctuates
driven
caring, nurturing, helpful
generally chill
like to learn new things !
gallery
Here's a few pics of me :)



My experience with
hodgkin's lymphoma (HL)
last update: 04/23/25
specifically classical HL,
subtype nodular sclerosis HL
(most common & curable type of HL)
for more information on hodgkin's lymphoma:
back to "about me" carrd:
my story
At first, I thought it was only an infection.
* my only symptoms:
• fatigue
• chronic cough (for months)
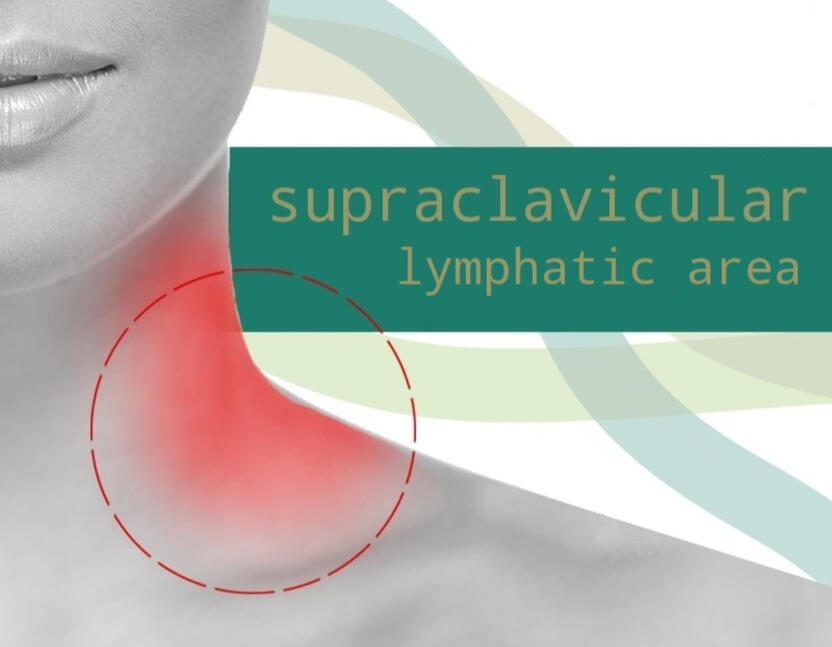
• lump on the inside of my neck
(supraclavicular lymph node)
Regular therapy (an antibiotic and steroid) seemed to help a bit - the symptoms lessened & even the lump felt smaller. However, it came back & the other symptoms came back.
* diagnosed on 9/1/22
at 25 years old
I'm an otherwise healthy individual. No other physical medical conditions.
* 1st PET scan verified advanced stage HL (stage 3)
10/31/22 was my last day at work before going on leave. Now too weak to work.
* 2nd PET scan (2 months after beginning treatment) shows NO activity
Hospital stay on 11/4 to 11/10 due to high resting heart rate (120 resting, 150 active) - it would not come down. I was also dehydrated and neutropenic (low neutrophils, a type of white blood cell = no immune system).
* 3rd PET scan (3 weeks after ending treatment) shows NO activity; remission
On 3/20/23, I find out treatment worked on my partner & I's 2 year anniversary <3
* CT scan (6 months after ending treatment) CONFIRMS & OFFICIALLY LABELS AS REMISSION
* STILL IN REMISSION AS OF 4/23/25
gallery





Diagnostic
blood work
(abnormalities):
6/29/22
- CRP (elevated)
- LDL Calc (elevated)
- monocyte # (elevated)
- neutrophil # (elevated)
- Non-HDL Chol (elevated)
- platelet count (elevated)
- WBC (elevated)
7/14/22
- WBC (elevated)
7/28/22
- A/G ratio (low)
- albumin (low)
- CRP (elevated)
- Globulin (elevated)
- HGB (low)
- IG # (elevated)
- iron saturation % (low)
- MCHC (low)
- MPV (low)
- neutrophil # (elevated)
- WBC (elevated)
8/25/22
- A/G ratio (low)
- AST (AGOT)
- Chloride (elevated)
- Globulin (elevated)
- WBC (elevated)
9/1/22
- AST (AGOT)
- Globulin (elevated)
- IG # (elevated)
- MCHC (elevated)
- monocyte # (elevated)
- MPV (low)
- neutrophil # (elevated)
- WBC (elevated)
DIAGNOSTIC IMAGING
SOFT TISSUE SONOGRAM
6/27/22
IMPRESSION:
right supraclavicular lymphadenopathy
1.8 x 1.6 x 2.3 cm symmetric ovoid hypoechogenicity. no fatty hilum. no necrosis or calcification.
CT SCANS
7/29/22

1. CHEST, ABDOMEN, AND PELVIS WITH CONTRAST
IMPRESSION:
1. Extensive lymphadenopathy within the chest most suggestive of lymphoma. There are a few prominent nodes in the upper
abdomen as well.
2. Borderline splenomegaly.
3. Hepatomegaly.
4. Two pulmonary nodules, the larger measuring 1 cm in the right lower lobe. These are indeterminate and while they could be
postinfectious/postinflammatory, pulmonary involvement with lymphoma or other malignant process difficult to fully excluded.
2. NECK SOFT TISSUE W CM
IMPRESSION:
1. Diffuse cervical lymphadenopathy with bulky right supraclavicular involvement concerning for lymphoma.
2. Oropharyngeal lymphoid tissue prominence, additional involvement versus reactive.
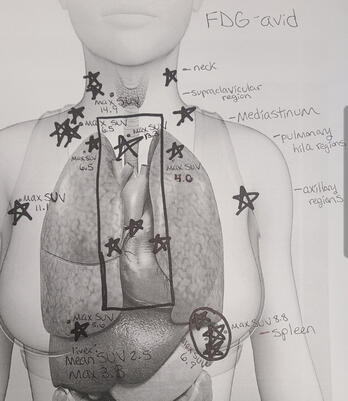
PET SCAN #1
9/14/22
IMPRESSION:
1. Extensive FDG-avid adenopathy at numerous nodal stations above the diaphragm. There is a single FDG-avid lymph node near
the splenic hilum compatible with nodal disease below the diaphragm.
2. There are numerous FDG-avid splenic lesions compatible with splenic lymphoma.
3. There are at least three FDG-avid bilateral pulmonary nodules compatible with pulmonary lymphoma.
4. Diffuse bone marrow activation is likely related to anemia, although strictly indeterminate.
staged as advanced HL (stage 3)
PROGNOSTIC IMAGING
PET SCAN #2
11/04/22
IMPRESSION:
1. Interval resolution of the majority of hypermetabolic abnormalities seen on the prior examination. Faint residual activity is noted
within RIGHT axillary nodes, corresponding to a Deauville score of 2. Additional nodes have decreased in size or resolved without
measurable residual tracer activity.
2. Hypermetabolic pulmonary and splenic abnormalities have resolved.
3. Diffuse bone marrow activation, likely related ongoing systemic therapy.
4. Stable appearance of small, symmetric, mildly FDG avid lymph nodes in the upper neck, favored to be reactive/inflammatory.
no activity - close to remission
PET SCAN #3
03/15/23
NO ACTIVITY (remission)
procedures
BIOPSY
(surgery)
8/25/22
! trigger warning !
somewhat graphic image
clinical report-conclusion:
The lymph node showed extensive replacement by thick collagen bands that
surround multiple variably sized cellular nodules with clusters of Hodgkin and
Reed-Sternberg cells. The H/RS-cells are positive for CD30 (membranous and
golgi), CD15, pax5 (dim); negative for B-cell markers CD20, CD79a, CD45, and
EBER-ISH. Given the characteristic staining pattern and mixed inflammatory cells
milieu, the cumulative findings are consistent with nodular sclerosing classic
Hodgkin lymphoma. The flow cytometric analysis identified increased (60.4%)
T-cells with a normal CD4:CD8 ratio of 2.7:1 and 34.4% polyclonal B-cells. This
correlates with the high number of small CD3-positive T-cells and scattered
reactive lymphoid follicles in the background demonstrated by IHC, respectively.

The results came back on 9/1/22,
confirming I had hodgkin's lymphoma
BONE MARROW SAMPLE
9/8/22
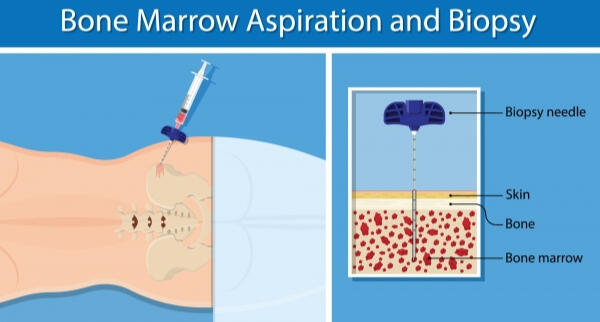
Note: Bone marrow aspiration and bone marrow biopsy can show whether your bone marrow is healthy and making normal amounts of blood cells.
MEDIPORT